HIGHLIGHTS
- Not all antibodies are the same, but they complement each other to protect us against infections
- Most vaccines aim to generate antibodies to fight infections
- B-cells and T cells are seen as the extension of human defences against the pandemic
- As more SARS-CoV-2 variants emerge, scientists are building up the body of knowledge about our collective defences
The new strains of coronavirus (SARS-CoV-2) have become a cause of concern when countries are rolling out large-scale vaccination programmes. The variants from Britain, Brazil, South Africa and the United States are reportedly partially resistant to the vaccines.
Recent reports of more infectious variants have had the alarm bells ringing. Among scientists, however, the new viral strains have spurred renewed interest in the responses from the “layers” of immunity, specifically by understanding the contributions of B cells and T cells to immunity. This has implications for treatments and vaccines.
What are antibodies? How do they boost immunity?
Antibodies (aka immunoglobulins) are the first line of defence. They are also known as “neutralising antibodies”, and are a key factor in the protection against SARS-CoV-2 infection. These large, Y-shaped proteins are used by our immune system to identify and “neutralise” viruses. It’s important to remember that the antibodies recognise a unique molecule of the pathogen (antigen).
Why are antibodies important?
Antibodies not only curb the severity of an illness but also prevents infection altogether. Antibodies, particularly those that bind to crucial viral proteins (such as the S protein in SARS-CoV-2), block infection, Dr Alessandro Sette, an immunologist at the La Jolla Institute for Immunology in California, told the journal Nature. They are seen as the key to “sterilising immunity”, either through vaccines or previous infection.
What’s the relationship between COVID-19 antibodies and vaccines?
Coronavirus vaccine development has largely focused on recognising the coronavirus spike protein and creating antibodies to neutralise the pathogen.
Protection by building up antibodies against specific viruses is considered the “gold standard”. But, it typically requires large numbers of antibodies to be generated.
What level of antibodies is required to gain protection against COVID-19?
Infections trigger the production of neutralising antibodies, measured in “titres”. A Nature article states that a minimum antibody titre of 1:40 confers enough protection from other respiratory infections such as influenza for at least 50 per cent of a given population. Any titre higher than 1:40 means higher levels of immunity.
What is an antibody test?
An antibody test screens for antibodies in the blood.
What are the standard antibody tests?
The presence or level of antibodies can be detected in a blood sample (serology) using tests such as plaque reduction neutralisation (PRNT) assay, or ELISA.
An antibody test does not check for the virus itself. Instead, it looks to see whether our immune system — our body’s response against infection — has kicked in.
How does an antibody test work?
A technician will take some blood, usually through a finger prick. The test looks for one or both kinds of antibodies to SARS-CoV-2, the virus that causes COVID-19:
IgM antibodies, which happen early in an infection
IgG antibodies, which are more likely to show up later

How are antibodies produced?
A human body makes antibodies when fighting an infection, like COVID-19. The same thing happens when we get a vaccine.
Are antibodies our only weapon against infections?
No. The absence of specific antibodies in blood samples does not necessarily mean an absence of immune memory, Nature stated in a new article. Other layers of defences exist within our immune system. In addition to antibody response, antigens (such as SARS-CoV-2) also trigger memory B cells and ‘killer’ T cells that seek and destroy infected cells.
Antibodies generated by previous infection or vaccination can become less effective. That’s the nature and function of antibodies.
If antibodies become less effective at fighting the disease, T cells could provide an additional weapon against COVID-19. Researchers are now poring through clinical data, looking for signs that T cells could provide lasting immunity.
How many mutations of SARS-CoV-2 are known? Which mutations are of utmost concern?
About 4,000. Viruses constantly evolve. The most prominent “variants of concern” are the ones from South Africa, the UK, Brazil and the US, according to Scientific American. But humans also evolve.
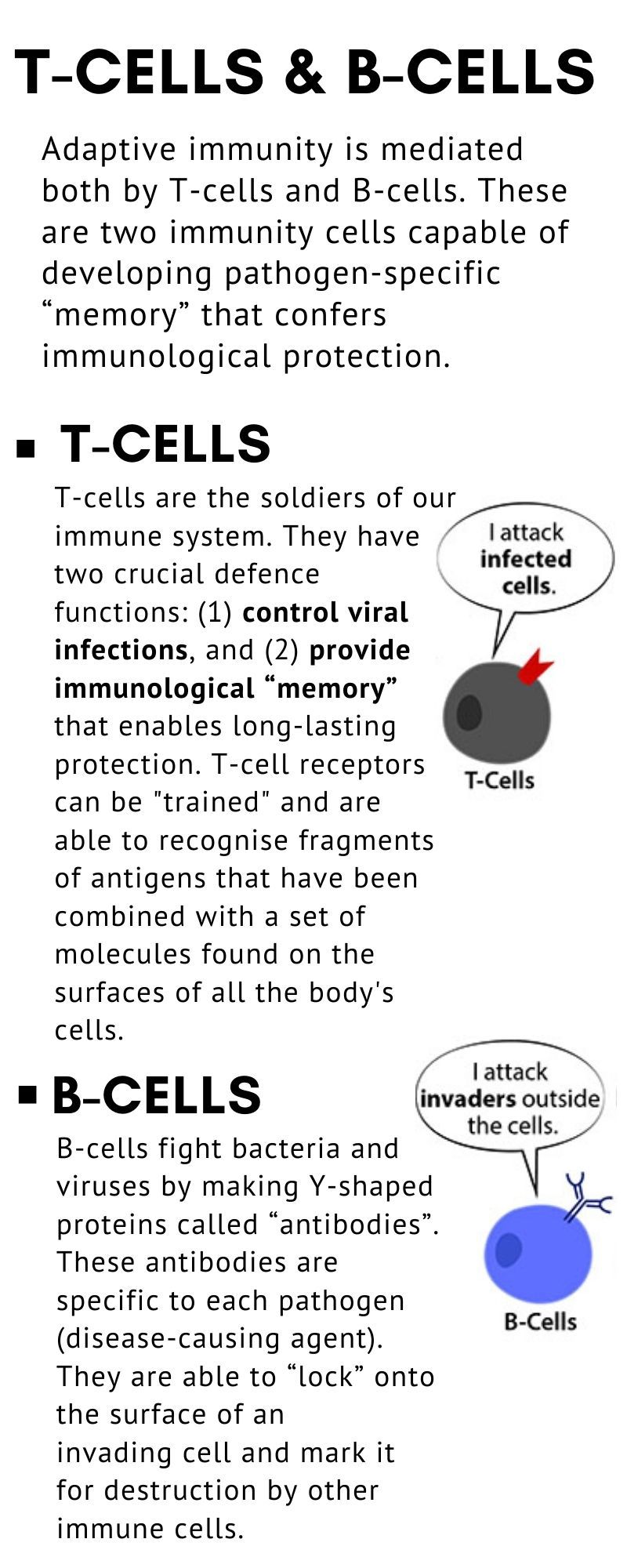
What’s the difference between antibodies, B cells and T cells? How do they help fight SARS-CoV-2 infection?
Antibodies: They are generated as part of our immune response within days of a viral infection, and are specific to the virus/antigen (or a variant).
B cells: Also called “memory” cells, they are part of our “adaptive immunity” and tend to remain longer and actively fight antigens in case of reinfections.
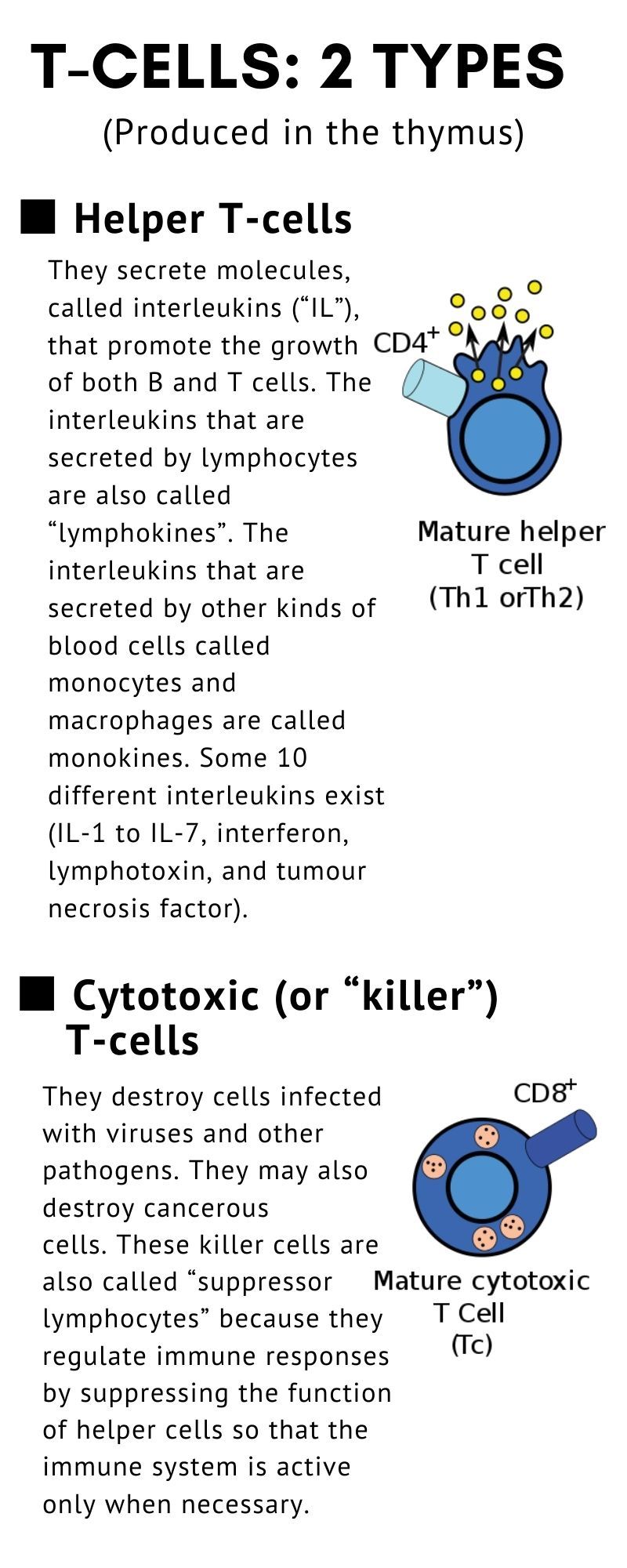
T cells: They are the so-called “warriors” against infectious diseases and are specific to active antigens. There are two types of T cells:
“Killer T cells” (or CD8+ T cells), likened to battalions that can target viruses. They search and destroy cells that are infected with the virus.
Helper T cells (or CD4+ T cells). They are important for various immune functions, including stimulating the production of antibodies and killer T cells.
Do T cells prevent infection?
No. T cells do not prevent infection. They, however, kick into action after a virus has infiltrated the body.
What is their function then?
T cells are important for clearing an infection that has already started, as they actively seek and destroy cells infected by a virus. However, specific T cell response elicited against SARS-CoV-2 can vary greatly between individuals, depending on age and so-called pro-inflammatory status.
What’s the role of T cells in mild or severe infections in the case of COVID-19?
They play a key role. Killer T cells could mean the difference between a mild infection and a severe one that requires hospital treatment, according to Nature.
“If they are able to kill the virus-infected cells before they spread from the upper respiratory tract, it will influence how sick you feel,” Annika Karlsson, an immunologist at the Karolinska Institute in Stockholm, Sweden, explained in the article.
T cells could also reduce transmission by restricting the amount of virus circulating in an infected person, meaning that the person “sheds” fewer virus particles into the community.
How long do these immune responses last?
Responses from different types of immunity agents vary. Specific antibodies immediately kick in within hours or days following a viral infection, memory B cells and specific T cells tend to last for months and even years, according to Nature Reviews Immunology.
What happens to T cell response in the case of severe COVID-19 cases?
Immunologists say that severe SARS-CoV-2 infection is usually a sign of T cell loss. This usually results in overdrive in the immune response of the host (patient), which then triggers massive or abnormal cytokine release (a phenomenon known as “cytokine storm”). This exaggerated immune response does nothing to clear the virus. Instead, it worsens respiratory distress, cardiac issues and may cause damage to other organs.
Experts led by Paola de Candia, believe that the response to SARS-CoV-2 infection partly depends on T cell memory. In an article in Trends in Immunology published in November 2020, the researchers said this memory is more pronounced in adults than children.
It is now known that deaths following SARS-CoV-2 infection are higher in older versus younger adults — and almost absent in children. The presence — or absence — of innate (antibodies) and adaptive immunity (B cells and T cells) depends on age and pre-existing comorbidities.
T cell response, or lack of it, determines the outcome of COVID-19 infection. An inappropriate immune response to an infection (known as immunopathology) leaves different collateral damage in COVID-19 patients, including death.
Is there evidence of greater T-cell resistance to SARS-CoV-2 and antibody resistance against new viral strains?
One study shows that T cells could be more resistant than antibodies to threats posed by emerging variants. Studies by Sette and his colleagues have shown that people who have been infected with SARS-CoV-2 typically generate T cells that target at least 15–20 different fragments of coronavirus proteins.
How are T cells identified?
T cells can be easily distinguished from other lymphocytes by the presence of a T-cell receptor (TCR) on their cell surface.
Which coronavirus proteins are targeted by memory T cells?
It’s not clear at this point. The coronavirus protein parts used as targets by memory T cells can vary widely from person to person. This would mean, researchers explain, that a population will generate a large variety of T cells that could be brought to bear against a virus. Unlike the situation for neutralising antibodies, it would be tough for the virus to mutate to escape cell recognition.
What are the South African, British, Brazil, and US variants called?
The SARS-CoV-2 variants identified in different places are:
- South Africa: 501Y.V2 (also called B.1.351).
- The British variant is called B.1.1.7
- The US variant is also known as B.1.1.7
- The Brazil variant is known as P1.
These variants are reportedly spreading rapidly in places where they have been detected.
How do these variants evade antibodies? And how do they react to memory T cells?
Lab tests showed that these variants are partially resistant to antibodies generated against previous coronavirus variants. Now researchers are investigating whether T cells could also cover such mutations. Early results of at least one new study suggest that this might be the case.
In one study, the researchers claimed to have found that most T-cell responses to coronavirus vaccination (or previous COVID-19 infection) do not target regions that were mutated in two recently discovered variants, including the South African strain.
Preliminary evidence shows that the vast majority of T-cell responses are unlikely to be affected by the mutations.
If T cell responses to the new variants work, what does that mean?
If T cells remain active against the South African variant, they might protect against severe disease, according to a Nature article, quoting immunologist John Wherry at the University of Pennsylvania in Philadelphia.
Data showing that T cells are “less vulnerable” to new variant are preliminary. So it’s hard to say if the same adaptive immune response can work against other strains. That means more investigations are needed to answer this question.
Are reports of the mutant viruses exaggerated?
Researchers have been analysing clinical-trial data for several coronavirus vaccines. The objective: establish whether or not their effectiveness “fades” in the face of new viral variants, especially the South African strain.
Nature reported that at least three vaccines — a protein vaccine made by Novavax (US), a single-shot vaccine made by Johnson & Johnson (US), and a vaccine made by AstraZeneca (UK) — were found “less effective” at protecting against mild COVID-19 in South Africa, where the 501Y.V2 variant dominates — than in countries where that variant is less common.
With AstraZeneca’s vaccine, it was found that the vaccine was only 22 per cent effective against mild COVID-19 in a sample of 2,000 people in South Africa.
There’s one criticism of that trial: the sample size was rather small, and its participants were too young to draw any conclusions about the severity of the disease, said Shane Crotty, an immunologist at the La Jolla Institute for Immunology.

How soon can new vaccines be made against new strains?
Based on our collective SARS-CoV-2 experience, a vaccine can be developed in one year, if not less — from DNA sequencing to a ready jab in a vial. Some coronavirus vaccine developers are already looking at ways to create next-generation vaccines that stimulate T cells more effectively.
California-based biotech company Gritstone is now designing an experimental shot incorporating genetic code for fragments of several coronavirus proteins known to elicit T-cell responses, as well as for the full spike protein. By design, it is hoped to generate a more robust antibody response. Nature reported that Gritsone’s clinical trials are set to start before April 2021.
The pandemic has increased collaboration among researchers. They have shared databases that allow for real-time tracking of viral mutations. Using DNA tests, which have now become routine, this will expose new variants. And new shots could potentially be arrayed against them sooner, instead of later.